

The anterior chamber (AC) is the aqueous humor-filled space inside the eye between the iris and the cornea's innermost surface, the endothelium.[1] Hyphema, anterior uveitis and glaucoma are three main pathologies in this area. In hyphema, blood fills the anterior chamber as a result of a hemorrhage, most commonly after a blunt eye injury. Anterior uveitis is an inflammatory process affecting the iris and ciliary body, with resulting inflammatory signs in the anterior chamber. In glaucoma, blockage of the trabecular meshwork prevents the normal outflow of aqueous humour, resulting in increased intraocular pressure, progressive damage to the optic nerve head, and eventually blindness.
The depth of the anterior chamber of the eye varies between 1.5 and 4.0 mm, averaging 3.0 mm. It tends to become shallower at older age and in eyes with hypermetropia (far sightedness). As depth decreases below 2.5 mm, the risk for angle closure glaucoma increases.
YouTube Encyclopedic
-
1/3Views:374 7923 6111 165
-
Development of Glaucoma Animation, Open Angle vs Angle Closure Glaucoma.
-
Vitreous humour
-
Eye Cubed Clinical Footage
Transcription
Glaucoma is a group of eye diseases in which the optic nerve is damaged leading to irreversible loss of vision. In most cases, this damage is due to an increased pressure within the eye. The eye produces a fluid called aqueous humor which is secreted by the ciliary body into the posterior chamber - a space between the iris and the lens. It then flows through the pupil into the anterior chamber between the iris and the cornea. From here, it drains through a sponge-like structure located at the base of the iris called the trabecular meshwork and leaves the eye. In a healthy eye, the rate of secretion balances the rate of drainage. In people with glaucoma, the drainage canal is partially or completely blocked. Fluid builds up in the chambers and this increases pressure within the eye. The pressure drives the lens back and presses on the vitreous body which in turn compresses and damages the blood vessels and nerve fibers running at the back of the eye. These damaged nerve fibers result in patches of vision loss, and if left untreated, may lead to total blindness. There are two main types of glaucoma: open-angle and angle-closure. Open-angle glaucoma , or chronic glaucoma, is caused by partial blockage of the drainage canal. The angle between the cornea and the iris is "open", meaning the entrance to the drain is clear, but the flow of aqueous humor is somewhat slow. The pressure builds up gradually in the eye over a long period of time. Symptoms appear gradually, starting from peripheral vision loss, and may go on unnoticed until the central vision is affected. Progression of glaucoma can be stopped with medical treatments, but part of vision that is already lost can not be restored. This is why it's very important to detect signs of glaucoma early with regular eye exams. Angle-closure glaucoma, or acute glaucoma, is caused by a sudden and complete blockage of aqueous humor drainage. The pressure within the eye rises rapidly and may lead to total vision loss quickly. Certain anatomical features of the eye such as narrow drainage angle, shallow anterior chamber, thin and droopy iris, make it easier to develop acute glaucoma. Typically, this happens when the pupil is dilated and the lens is stuck to the back of the iris. This prevents the aqueous humor from flowing through the pupil into the anterior chamber. Accumulation of fluid in the posterior chamber presses on the iris causing it to bulge outward and block the drainage angle completely. Acute angle-closure glaucoma is a medical emergency and requires immediate attention.
Clinical significance
Depth measurement
Determining the anterior chamber depth (ACD) is important in estimating the risk of angle closure glaucoma. There are various method of measuring ACD, including examination through a slit lamp, ultrasound and Scheimpflug photography. These methods require sophisticated examination equipment and expertise.
A simpler clinical method of quantitatively estimating ACD using smartphone photography (EZ ratio) was developed by Dr Ehud Zamir from the Centre for Eye Research Australia, the University of Melbourne, and published in 2016.[2]
EZ ratio method
The EZ ratio method is one way to calculate the estimated anterior chamber depth.[2] To start, the patient looks at a target in the distance with one eye covered. The examiner takes a digital photograph of the open, examined eye, from the side, perpendicular to the visual axis (a profile photograph).
The following parameters then need to be measured in the photograph, using a personal computer or a smartphone (figures 1,2):
1. The pixel distance between the limbus (the junction between clear cornea and white sclera) and the front of the cornea. This distance is referred to as Z.
2. The pixel distance between the limbus and the centre of the pupil. This distance is referred to as E.
E:Z ratio is the arithmetic ratio between E and Z.
This ratio is linearly correlated with the depth of the anterior chamber with the following equation:
Anterior chamber depth (expressed in millimetres) = -3.3 x EZ ratio + 4.2
This estimate has been shown to be accurate with a 95% confidence interval of +/– 0.33 mm error, when compared to measurements of the anterior chamber depth by Scheimpflug photography.[2]


Associated immune deviation
One peculiar feature of the anterior chamber is dampened immune response to allogenic grafts. This is called anterior chamber associated immune deviation (ACAID), a term introduced in 1981 by Streilein et al.[3][4] This phenomenon is relevant to the fact that the eye is considered an "immune privileged site", like the brain and the testis.
Pathology
Additional images
-
 Anterior chamber angle cross-section imaged by an SD-OCT.
Anterior chamber angle cross-section imaged by an SD-OCT. -
 Gonioscopy of the anterior chamber angle
Gonioscopy of the anterior chamber angle -
 Gonioscopy of the anterior chamber angle. Labeled structures: 1. Schwalbe's line, 2. Trabecular meshwork (TM), 3. Scleral spur, 4. Ciliary body, 5. Iris
Gonioscopy of the anterior chamber angle. Labeled structures: 1. Schwalbe's line, 2. Trabecular meshwork (TM), 3. Scleral spur, 4. Ciliary body, 5. Iris -
 Anterior chamber IOL
Anterior chamber IOL -
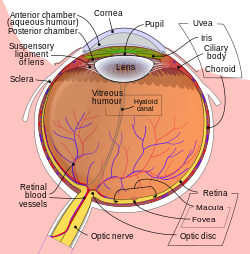
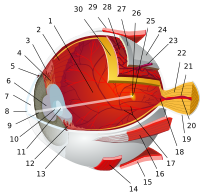
 Structures of the eye labeled
Structures of the eye labeled -
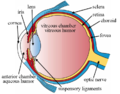
 This image shows another labeled view of the structures of the eye
This image shows another labeled view of the structures of the eye




See also
References
- ^ Cassin, B.; Solomon, S. (1990). Dictionary of eye terminology. Gainesville, Fla: Triad Pub. Co. ISBN 978-0-937404-33-1.
- ^ a b c Zamir, Ehud (2016). "A novel method of quantitative anterior chamber depth estimation using temporal perpendicular digital photography". Translational Vision Science & Technology. 5 (4): 10. doi:10.1167/tvst.5.4.10. PMC 4981489. PMID 27540496.
- ^ Streilein JW, Niederkorn JY (May 1981). "Induction of anterior chamber-associated immune deviation requires an intact, functional spleen". J. Exp. Med. 153 (5): 1058–67. doi:10.1084/jem.153.5.1058. PMC 2186172. PMID 6788883.
- ^ "Research Story - sce.com". Archived from the original on 2015-02-11. Retrieved 2012-07-16.
External links
- Atlas image: eye_2 at the University of Michigan Health System - "Sagittal Section Through the Eyeball"
| Fibrous tunic (outer) |
|  | |||||
|---|---|---|---|---|---|---|---|
| Uvea / vascular tunic (middle) |
| ||||||
| Retina (inner) |
| ||||||
| Anatomical regions of the eye |
| ||||||
| Other | |||||||
| National | |
|---|---|
| Other | |